A Preventable Setback: Measles Resurgence and the Risk to U.S. Elimination Status
Christina Sellers, Stephen M. Modell, Marcia Ditmyer

We would love to hear from you!
Make your voice heard by advocating for public health matters:
MPHA is seeking Board nominees for the 2026-2028 term:
After nearly 30 years of keeping measles at bay, the United States now stands on the brink of losing one of its most significant public health achievements. The return of measles is no longer a theoretical concern—it is unfolding in real time. In January 2026, after nearly three decades, the United States is expected to lose its measles elimination status.
As of December 23, 2025, a total of 2,065 confirmed measles cases had been reported nationwide.¹ Alarmingly, 68% of these cases (n = 1,402) occurred among children and adolescents from birth to 19 years of age, with more than one-quarter (26%, n = 537) affecting children under the age of five—those most vulnerable to severe complications 1.
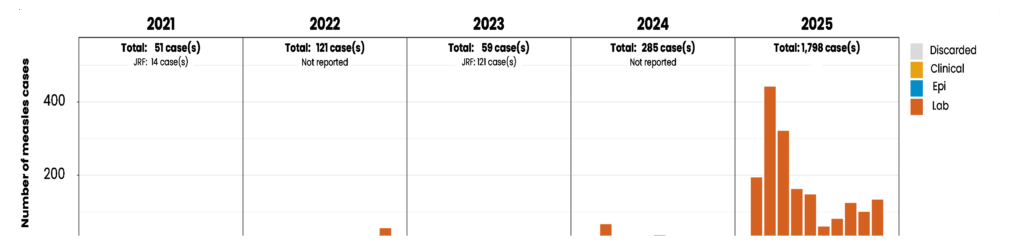
Table 1 illustrates the dramatic rise in measles cases year to date, highlighting a sharp and concerning trend. By March 2025, the number of confirmed cases had already surpassed the total reported for all of 2024, representing a staggering 625% increase.¹ Figure 1 further demonstrates the sustained and accelerating rise in measles incidence since 2021.²
Together, these data underscore a sobering reality: measles has reestablished a foothold in the United States. What was once a rare, preventable disease is once again circulating in communities—placing infants, children, and unvaccinated individuals at growing risk and signaling a dangerous erosion of decades of public health progress.
| Year | Total Confirmed Cases | Outbreaks Reported |
| 2024 | 285 | 16 |
| 2025 | 2,065 | 50 |
NOTE: CDC, 2026
There have also been 49 measles outbreaks reported in 2025.1 An outbreak is declared when there are 3 or more genetically-linked cases in the chain of transmission. 1,3 Of the reported measles cases, 1,820 (88%) of cases are outbreak-associated with the Texas outbreak originating in January of 2025.1
Of reported cases, 93% of those who have been infected have been unvaccinated or have an unknown vaccination status.1 In 2025, Michigan experienced such outbreaks in Grand Traverse and Montcalm Counties (MDHHS 2025).4
Measles Elimination Status to Be at Risk—and How Did We Get Here?
Measles is a highly contagious viral disease spread through the air when an infected person breathes, coughs, or sneezes.⁵ The consequences of infection can be severe. In 2024 alone, approximately 12% of reported measles cases required hospitalization, and three deaths occurred—two of them among children. 1,⁶ Measles can also lead to encephalitis, a serious inflammation of the brain that occurs in approximately 1 in 1,000 cases.⁶ In addition, nearly everyone infected with measles experiences some degree of immune “amnesia,” a condition that weakens immune memory and leaves individuals vulnerable to other infectious diseases for years after recovery.⁶–⁷
Measles elimination status is determined by national public health authorities, including the Centers for Disease Control and Prevention (CDC), in coordination with international partners such as the Pan American Health Organization (PAHO) and the World Health Organization (WHO). The United States regularly reports data on measles cases, viral genotypes, outbreaks, and prevention efforts to these organizations. If continuous, genetically linked measles transmission—referred to as endemic measles—persists for 12 consecutive months, a country’s elimination status is revoked.⁸
The loss of measles elimination status would signal a major public health setback. It would mean a sustained increase in measles transmission, greater strain on the healthcare system, rising healthcare costs, and a reversal of decades of public health progress.⁹ For everyday Americans, this would translate into a new and unsettling reality—where a routine trip to the grocery store, a classroom visit, or a child’s playdate could carry the risk of exposure to a highly contagious and potentially deadly disease, particularly for those who are unvaccinated or medically vulnerable.
The United States’ Journey to Elimination
Routine measles vaccination in the United States began in 1967, with the first dose administered to infants at 12 months of age.10 Although vaccination initially led to a substantial decline in measles cases, outbreaks continued to occur. In response, the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices (ACIP) recommended the addition of a second dose of the measles-mumps-rubella (MMR) vaccine in 1989, to be administered prior to school entry. 10 This two-dose schedule is supported by extensive scientific evidence, despite recent calls by the current administration to divide the vaccine into separate components.11
The implementation of the two-dose MMR schedule, combined with school vaccination requirements and removal of financial barriers through the Vaccines for Children (VFC) program, resulted in a dramatic decline in measles cases nationwide. Between 1993 and 2001, measles incidence fell sharply, culminating in the United States being declared measles-free in 2000. 9 Since that time, the U.S. has maintained elimination status; however, this achievement is increasingly at risk. Concerns have emerged that funding for the VFC program may be reduced under current federal budget proposals, threatening access to routine childhood immunizations.12
In 2018–2019, the United States experienced significant measles outbreaks. During the 2019 outbreak alone, approximately 1,250 cases were reported across 31 states.3, 9 Sustained transmission nearly resulted in the loss of elimination status, but aggressive public health interventions and vaccination efforts successfully interrupted transmission before the 12-month threshold was reached. The 2019 outbreak represented the largest measles outbreak since elimination was achieved in 2000—until the current resurgence in 2025.1, 13
Vaccination remains the most effective public health intervention for preventing measles and other vaccine-preventable diseases.5 Despite this, vaccination coverage in the United States has steadily declined and now falls well below the 95% threshold required for herd immunity.6 A 2025 study published in The Journal of the American Medical Association reported that national two-dose MMR coverage declined from 93.92% prior to the COVID-19 pandemic to 91.26% in the post-pandemic period.14
State-level data reveal even greater concern. In Michigan, as of September 2025, only 78% of preschool-aged children had received one dose of MMR, and just 86% of adolescents aged 13–17 had completed the two-dose series.15 These rates fall well below the threshold required to prevent sustained transmission, placing Michigan communities at elevated risk for future outbreaks.
Vaccine hesitancy remains a significant barrier to immunization uptake, fueled largely by misinformation and disinformation propagated through social media platforms.16–18 Persistent concerns—particularly the false belief that the MMR vaccine causes autism—continue to influence parental decision-making, despite overwhelming scientific evidence disproving this claim.19 The American Academy of Family Physicians has explicitly encouraged clinicians to reassure families about vaccine safety and address misinformation directly.20
Stopping the Backslide
Urgent action is needed to reverse declining vaccination rates and protect public health. The American Academy of Pediatrics (AAP) supports medical exemptions only when clinically justified and determined on an individual basis.21 The AAP further recommends that states eliminate non-medical exemptions to school immunization requirements and implement safeguards to ensure that any medical exemptions are evidence-based and appropriately applied. 21 Because only a small percentage of children have legitimate medical contraindications to vaccination, these policy changes would have a substantial impact on improving population-level immunity without placing undue burden on families.22
Historical precedent demonstrates that strong immunization policies are effective in preventing measles transmission. 10 Restoring and maintaining high vaccination coverage will require coordinated policy action at the state level, including eliminating non-medical exemptions in Michigan. At the federal level, healthcare providers and public health professionals must advocate for continued funding of the Vaccines for Children program, which remains a cornerstone of equitable vaccine access.23
Equally important are effective communication strategies. Parents benefit from open, respectful, and nonjudgmental conversations with trusted healthcare providers regarding vaccine safety and efficacy.10 Evidence suggests that vaccination education is most effective when initiated during pregnancy and reinforced at every well-child visit throughout early childhood.5,10,18,24 Reminder and recall systems for vaccinations and well-child visits have also been shown to improve immunization rates.10
Together, these strategies—strong policy, consistent access, trusted communication, and early education—represent the most effective path forward to protect children, preserve measles elimination status, and prevent the re-emergence of a disease that is both preventable and potentially deadly.
Footnote: While writing this article, an additional 153 cases were added in a matter of 3 weeks (December 9 to December 31).
References:
- Centers for Disease Control and Prevention (CDC). U.S. Measles Cases 2025. Retrieved January 2, 2026 from Measles Cases and Outbreaks | Measles (Rubeola) | CDC.
- World Health Organizations (WHO). Measles Global Update, December 2025. Retrieved January 2, 2026 from WHO updates data on measles outbreaks each month
- Morbidity and Mortality Weekly Report (MMWR), Centers for Disease Control and Prevention (CDC). National Update on Measles Cass and Outbreaks – U.S. January 1 – October 1, 2019). Released October 4, 2019. Retrieved January 2, 2026 from National Update on Measles Cases and Outbreaks — United States, January 1–October 1, 2019 | MMWR.
- Michigan Department of Health and Human Services. (2025). Updates on Measles in the State of Michigan. Retrieved December 31, 2025, from Measles Updates.
- World Health Organization (WHO). Measles: Key Facts, 2025, Nov. Retrieved January 2, 2026 from Measles.
- Committee on Infectious Diseases, American Academy of Pediatrics. Red Book: 2024-2027 Report of the Committee on Infectious Diseases (33rd Edition). Edited by Kimberlin DW et al. April 2024: American Academy of Pediatrics DOI: https://doi.org/10.1542/9781610027373. Retrieved January 2, 2026 from https://publications.aap.org/redbook/book/755/chapter/14079321/Measles
- Mina MJ, Kula T, Leng Y, Li M, de Vries RD, Knip M, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science 2019;366:599-606. Retrieved January 2, 2026 from https://www.jpeds.com/article/S0022-3476%2819%2931728-7/fulltext
- Measles and Rubella Elimination Regional Monitoring and Re-Verification Commission. Pan American Health Organization, World Health Organization, Americas Region. Measles and Rubella Elimination Regional Monitoring and Re-Verification Commission. How is a country re-verified after an outbreak? Retrieved January 2, 2026 from Measles and Rubella Elimination Regional Monitoring and Re-Verification Commission – PAHO/WHO | Pan American Health Organization.
- American Academy of Pediatrics. With measles elimination status at risk, pediatricians are ‘most important line of defense.’ 2025, Nov. Retrieved January 2, 2026 from With measles elimination status at risk, pediatricians are ‘most important line of defense’ | AAP News | American Academy of Pediatrics.
- Jackson, MA, Harrison C. On the Brink: Why the U.S. is in Danger of Losing Measles Elimination Status. Mo Med, 2019 Jul-Aug;116(4):260–264. Retrieved January 2, 2026 from https://pmc.ncbi.nlm.nih.gov/articles/PMC6699811/
- Czopek M, Why the measles, mumps and rubella vaccine is combined. Retrieved December 31, 2025, from https://www.politifact.com/article/2025/oct/31/MMR-vaccine-combination-trump-separate.
- Turner W, RFK Jr.’s new regime puts vaccine coverage for low-income children in jeopardy. Retrieved December 31, 2025, from https://healthlaw.org/rfk-jr-s-new-regime-puts-vaccine-coverage-for-low-income-children-in-jeopardy.
- IVAC International Vaccine Access Center. Johns Hopkins Bloomberg School of Public Health. U.S. Measles Cases Hit Highest Level Since Declared Eliminated in 2000. Published July 7, 2025. Retrieved January 2, 2026 from U.S. Measles Cases Hit Highest Level Since Declared Eliminated in 2000 | International Vaccine Access Center.
- Dong E. Salyed S, Nearchou A. et al. Trends in County-Level MMR Vaccination Coverage in Children in the U.S. JAMA, 2025, June 2, 334(8), doi:10.1001/jama.2025.8952. Retrieved January 2, 2026 from https://jamanetwork.com/journals/jama/fullarticle/2834892
- Michigan Department of Health and Human Services (MDHHS). Michigan’s Statewide Quarterly Immunization Report Card. Retrieved January 2, 2026 from State_Level_ReportCard.pdf.
- Institute for Vaccine Safety. Johns Hopkins Bloomberg School of Public Health. Do Vaccines Cause Autism? Retrieved from January 2, 2026 Do Vaccines Cause Autism? – Institute for Vaccine Safety.
- Novilla MLB, Goates MC, Redelfs AH, et al. Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy. Vaccines (Basel). 2023 May 2;11(5):926. doi: 10.3390/vaccines11050926. PMID: 37243030; PMCID: PMC10224336. Retrieved January 2, 2026 from https://pmc.ncbi.nlm.nih.gov/articles/PMC10224336/
- O’Leary ST, Opel DJ, Catalki JR, et al. Strategies for improving vaccine communication and uptake, Pediatrics (2024) 153 (3): e2023065483. https://doi.org/10.1542/peds.2023-065483
- Institute for Vaccine Safety, Johns Hopkins Bloomberg School of Public Health. Do vaccines cause autism? Updated May 19, 2025. Retrieved January 2, 2026 from Do Vaccines Cause Autism? – Institute for Vaccine Safety.
- American Academy of Family Physicians. (2025). Measles Vaccine. Retrieved December 31, 2025, from https://www.aafp.org/family-physician/patient-care/prevention-wellness/immunizations-vaccines/disease-pop-immunization/measles-vaccine.html.
- Haskell JM, Brothers K, Bode S, et al. Medical vs Nonmedical Immunization Exemptions for Child Care and School Attendance: Policy Statement. Pediatrics (2025) 156 (2): e2025072714. Retrieved January 2, 206 from https://doi.org/10.1542/peds.2025-072714
- Seither R, Yusuf OB, Dramann D, Calhoun K, Mugerwa-Kasujja A, Knighton CL. Coverage with selected vaccines and exemption from school vaccine requirements among children in kindergarten—United States, 2022–23 school year. MMWR Morb Mortal Wkly Rep. 2023;72(45):1217–1224. PubMed doi: 10.15585/mmwr.mm7245a2.
- Children’s Hospital of Philadelphia. (2025). Technically speaking: 5 avenues for vaccine advocacy. Retrieved January 1, 2025, from https://www.chop.edu/vaccine-update-healthcare-professionals/newsletter/5-avenues-vaccine-advocacy.
- Frew PM, Lutz CS. Interventions to increase pediatric vaccine uptake: An overview of recent findings. Hum Vaccin Immunother. 2017 Nov 2;13(11):2503-2511. doi: 10.1080/21645515.2017.1367069. Epub 2017 Sep 26. PMID: 28949819; PMCID: PMC5703404. Retrieved January 2, 2026 from https://pmc.ncbi.nlm.nih.gov/articles/PMC5703404/
- O’Leary ST, Opel DJ, Catalki JR, et al. Strategies for improving vaccine communication and uptake, Pediatrics (2024) 153 (3): e2023065483. https://doi.org/10.1542/peds.2023-065483
Updated 01/12/2026