Heart Health Month — February is American Heart Month
Marcia Mastracci Ditmyer, PhD, MBA, MS; Stephen M Modell, MD, MS; Richard Douglass, MPH, PhD

Heart Disease in the United States: Why It Matters
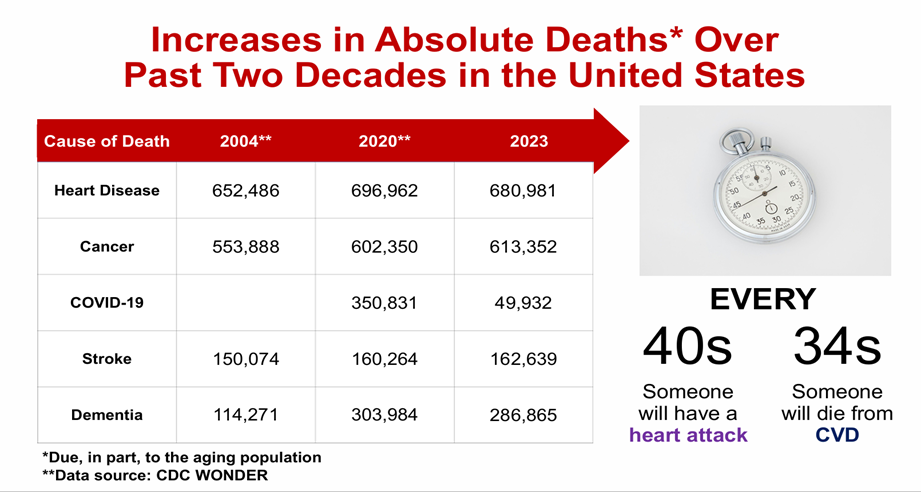
Heart disease remains the leading cause of death in the United States for both men and women, far surpassing all other causes.¹˒² In 2023 alone, more than 919,000 deaths were attributed to cardiovascular disease—approximately 1 in every 3 deaths nationwide.¹˒² Notably, nearly 1 in 6 cardiovascular deaths occurs among adults younger than 65, underscoring that heart disease is not limited to older populations.¹˒² Coronary heart disease, the most common form, accounted for more than 370,000 deaths in 2022, and someone in the U.S. experiences a heart attack about every 40 seconds.¹˒² These sobering figures highlight why prevention, early detection, and lifestyle change remain central public health priorities.
We would love to hear from you!
Make your voice heard by advocating for public health matters:
MPHA is seeking Board nominees for the 2026-2028 term:
Beyond mortality, heart disease imposes a substantial burden through chronic illness, disability, and economic costs. Approximately 5% of adults aged 20 and older report having coronary artery disease. Each year, about 805,000 people in the United States experience a heart attack, including 605,000 first events and 200,000 recurrent events among individuals with a prior history.¹˒³˒⁴ The lifetime cost of cardiovascular disease—including direct health care expenses and lost productivity—totals hundreds of billions of dollars annually.
In recognition of this burden, the United States designates February as American Heart Month, a national observance aimed at raising awareness, promoting prevention strategies, and encouraging individuals to “know their numbers,” including blood pressure, cholesterol, and blood glucose levels.
The financial impact of cardiovascular disease is projected to worsen. The annual cost of care, including health care expenditures and lost productivity, is expected to rise from $634 billion in 2022 to nearly $2 trillion by 2050, making cardiovascular disease the costliest chronic condition in the nation.⁴ Figure 1 (American Heart Association) illustrates the steady increase in absolute cardiovascular deaths in the U.S. over the past two decades.
Heart Health in Michigan: A Local Perspective
Heart disease does not affect only the nation—it has a profound impact here in Michigan. According to state health data, heart disease has been the leading cause of death in Michigan for more than a decade, consistently exceeding deaths from cancer and unintentional injuries.6,7
In 2023, more than 26,000 Michigan residents died from heart disease, making it the single largest cause of death statewide.⁶ Michigan’s interactive cardiovascular disease dashboard provides detailed snapshots of disease prevalence, mortality, and risk factors among Michigan adults (Figure 2 example).6 Hospitalization data further demonstrate a significant burden, with high age-adjusted discharge rates for major cardiovascular conditions—such as coronary heart disease and heart failure—particularly among older adults.7 These patterns emphasize the need for sustained heart health awareness and prevention efforts across both urban and rural communities throughout the state.

Awareness Activities: Wear Red and Spread the Word

During Heart Month, communities nationwide participate in National Wear Red Day, observed on the first Friday in February. On this day, individuals are encouraged to wear red to increase visibility and awareness of heart disease—especially among women.8 Sponsored by the National Heart, Lung, and Blood Institute (NHLBI) and partner organizations, Wear Red Day highlights that heart disease is the leading cause of death among women, despite many being unaware of their personal risk. This initiative is part of broader national efforts to improve cardiovascular health literacy and promote preventive action.
Heart Health Is Preventable — Get Involved
Heart disease risk is influenced by a combination of factors, including high blood pressure, high cholesterol, smoking, poor diet, and physical inactivity. Many of these risk factors are modifiable, meaning that steps taken today can significantly reduce future disease risk and improve overall quality of life.
Know the Risk Factors!
The non-medical drivers of health and the human environments of our lives interact profoundly with individual risk factors for cardiovascular disease (CVD) and heart attacks. When these factors are addressed together, public health and clinical efforts create the greatest opportunity for meaningful, sustained improvements in individual and community health. Table 1 outlines these drivers. Roughly three-quarters of health outcomes are associated with non-medical drivers of health, while medical care and genetics together account for about one-quarter. This distribution explains why clinical care alone—without addressing housing, food, transportation, income, and social conditions—has limited ability to improve long-term cardiovascular outcomes at the population level. While genetics and medical care remain important, the majority of cardiovascular disease risk is shaped by non-medical drivers of health, underscoring the need for integrated clinical, public health, and community-based strategies.
Table 1. Interaction of Medical, Non-Medical, and Genetic Drivers
| Category | Risk Factor | How It Increases CVD / Heart Attack Risk |
| Non-Medical Drivers (Social Determinants & Human Environments) Accounts for ~70%-80% | Housing insecurity & substandard housing | Poor insulation and heating increase energy costs, reduce disposable income, and force tradeoffs between food, medications, and care; indoor air pollution worsens co-morbidities like COPD, increasing CVD risk. |
| Social isolation (urban & rural) | Increases depression, reduces physical activity, delays detection of acute events, and limits social support during crises; physical barriers (stairs, snow removal) can trigger cardiac events. | |
| Transportation barriers (EMS & NEMT) | Delayed emergency response increases mortality; lack of non-emergency medical transportation limits access to chronic disease management and follow-up care. | |
| Poverty & financial insecurity | Forces cost-based decisions that deprioritize nutrition, medications, and preventive care; lack of retirement security increases stress in older age when CVD risk is highest. | |
| Food deserts/limited access to nutritious food | Reliance on gas stations or dollar stores increases intake of sodium, sugar, and ultra-processed foods associated with CVD. | |
| Socio-cultural habits & norms | Cultural acceptance of tobacco, alcohol, poor diet, and sedentary lifestyles (including retirement patterns) normalizes behaviors that elevate CVD risk. | |
| Minimum wage work & multiple jobs | Time scarcity limits exercise, healthy eating, medical visits, and adherence to treatment plans; chronic stress increases cardiovascular risk. | |
| Aging population & workforce shortages | Higher concentration of older adults raises community-level CVD prevalence while healthcare workforce shortages reduce access to timely care, especially in rural areas. | |
| Chronic stress & perceived insecurity | Financial strain, unsafe environments, and job instability contribute to sustained physiologic stress responses linked to CVD. | |
| Medical Drivers (Clinical & Behavioral) Accounts for ~10%-20% | Hypertension | Chronically elevated blood pressure damages arterial walls and accelerates atherosclerosis. |
| Hyperlipidemia (high LDL, low HDL) | Promotes plaque formation and coronary artery blockage. | |
| Diabetes / insulin resistance | Increases inflammation, vascular damage, and accelerates coronary disease. | |
| Tobacco use (smoking, vaping) | Causes endothelial damage, increases clotting, and promotes atherosclerosis. | |
| Obesity | Associated with hypertension, diabetes, dyslipidemia, and systemic inflammation. | |
| Physical inactivity | Reduces cardiovascular fitness and worsens metabolic risk factors. | |
| Poor diet (high sodium, sugar, ultra-processed foods) | Contributes to hypertension, obesity, and dyslipidemia. | |
| Excess alcohol use | Raises blood pressure, triglycerides, and cardiomyopathy risk. | |
| COPD and other chronic lung disease | Increases cardiac workload and hypoxia, raising CVD event risk. | |
| Poor medication adherence | Leads to uncontrolled chronic disease and increased cardiac events. | |
| Genetic & Biological Drivers Accounts for ~10%-20% | Family history of CVD | Inherited predisposition to atherosclerosis, hypertension, or cardiomyopathy. |
| Genetic lipid disorders (e.g., familial hypercholesterolemia) | Markedly elevated cholesterol levels independent of lifestyle factors. | |
| Genetic predisposition to hypertension or diabetes | Increases baseline risk even before environmental or behavioral exposures. | |
| Age | Risk increases with advancing age due to cumulative vascular damage. | |
| Sex & biological factors | Differences in risk profiles, symptom presentation, and outcomes between sexes. |
Know Your Risk Numbers
- Get regular screenings for blood pressure, cholesterol, and blood sugar. Take the Henry Ford Health 5-minute Heart Smart Quiz to explore your personal risk factors.13
- Understand how age, family history, and lifestyle affect your heart health. Visit the MI Genetics Resource Center website to explore tools to assess your family health history.14
Make Healthy Lifestyle Choices
- Follow a heart-healthy diet rich in fruits, vegetables, and whole grains.
- Aim for at least 150 minutes of moderate physical activity per week.
- Quit smoking and avoid exposure to secondhand smoke.
Support Your Community
- Encourage friends, family, and coworkers to learn about heart health.
- Participate in local awareness events or health screenings during Heart Month.
Take Action Today
Heart disease can be prevented, controlled, and managed when individuals and communities take informed action. This February — and every day — check your risk, talk to your health care provider, and take small but powerful steps toward better heart health. Your heart matters.
References
- Centers for Disease Control and Prevention. Heart Disease Facts. Heart Disease in the United States. Retrieved January 25, 2026, from Heart Disease Facts | Heart Disease | CDC.
- National Center for Health Statistics. Multiple Cause of Death 2018–2023 on CDC WONDER Database. Accessed February 1, 2025. https://wonder.cdc.gov/mcd.html
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Circulation. 2023;147:e93–e621.
- National Institute of Health Care Management (HIHCM) Foundation. Growing Budget on Chronic Diseases. 2025. Retrieved January 25, 2026 from The Growing Burden of Chronic Diseases.
- American Heart Association. 2026 heart disease and stroke statistics update. 2023 deaths in the United States. Retrieved January 25, 2026 from 2026 American Heart Association Statistics Overview.
- Michigan Department of Health and Human Services. Cardiovascular Disease Epidemiology. Retrieved January 25, 2026 from Cardiovascular Disease Epidemiology.
- Michigan Department of Health and Human Services. Cardiovascular-Related Hospitalization among Michigan Adults – 2017. Retrieved January 25, 2026 from Cardiovascular-Related Hospitalization among Michigan Adults – 2017.
- National Heart, Lung, and Blood Institute. National Wear Red Day® & American Heart Month. Retrieved January 25, 2026 from National Wear Red Day® & American Heart Month | NHLBI, NIH.
- National Academies of Sciences, Engineering, and Medicine. Communities in action: Pathways to health equity. The National Academies Press. 2017. https://doi.org/10.17226/24624
- Centers for Disease Control and Prevention. Why is addressing social determinants of health important? CDC website. Updated July 2024. Retrieved on January 26, 2026 from
https://www.cdc.gov/about/priorities/why-is-addressing-sdoh-important.html - Schneider EC.Let’s get it right: Consistent measurement of drivers of health. Commonwealth Fund. November 2023. Retrieved on January 26, 2026 from https://www.commonwealthfund.org/blog/2023/lets-get-it-right-consistent-measurement-drivers-health.
- Ganatra S, Dani SS, Shah S, et al.Social determinants of health and their impact on cardiovascular disease outcomes. J Am Heart Assoc. 2024;13(4):e030486. doi:10.1161/JAHA.123.030486
- Henry Ford Health. Heart Smart Quiz. Retrieved January 25, 2026 from https://www.henryford.com/campaign/heart-health?
- MI Genetics Resource Center. Family Health History. Retrieved January 25, 2026 from https://migrc.org/providers/family-health-history.
Updated 01/26/2026